_191119034350.jpg)
Glossary
bias – Any systematic error in an epidemiologic study that results in an Incorrect estimate of the association between exposure end risk of disease.
cause-and-effect relationship – Positive criteria in judging causality which include: strength of association, biologic credibility, consistency of findings, as well as, temporal sequence and dose response relationships.
chance – A happenstance; an occurrence that happens by being lucky or unlucky.
cohort – A subgroup sharing a common factor in a statistical survey.
confounding factors – Conditions that are lumped together with other conditions Indiscriminately.
epidemiology – All the elements contributing to the occurrence or non-occurrence of a disease in a population.
etiological agents – The agent(s) of c~use or origin for a specific disease.
excess cancers – A statistically significant higher number of cancer cases in comparison to the number of expected cancer cases in the general population.
linear energy transfer (LEI). low and high – The average amount of energy lost per unit track length. Low-LET is characteristic of light charged particles such as electrons produced by x- and γ where the distance between ionizing events is large on the scale of a cellular nucleus. High-LET Is characteristic of heavy charged particles such as protons and α-particles where the distance between ionizing events is small on the scale side of a cellular nucleus.
morbidity – The rate of disease or proportion of diseased persons in a given locality.
mortality – The death rate from a particular disease or proportion of deaths to the population of a given locality.
prospective study – A type of observational epidemiologic study where exposure has occurred in the past and the subject is observed to see if disease develops from the past exposure compared to non-exposed individuals. (Referred to as a cohort study by some.)
retrospective study – A type of observational epidemiologic study where exposure and disease has occurred in the past and the subject is reviewed to see if the exposure caused the disease when compareed to non-exposed individuals with the same disease. (Referred to as a case-control study by some.)
Introduction
Much debate rages concerning chronic low-dose radiation exposure. This brief literature summary focuses on the historical aspects of that debate and more recent reports on the controversy. Certainly, the advantages of continued vigilance on chronic low-dose radiation exposure cannot be denied. A possible answer should be provided for the ongoing question of what, if any, causality is associated with low-dose radiation exposure so that radiation workers can have “peace of mind”, and to settle any liability issues associated with low-dose radiation exposure.
Also, the question arises whether or not strict adherence to radiation safety is necessary if no clinically measurable effects arc occurring in chronic low-dose occupationally exposed individuals. A short set of criteria for further study is explored. This retrospective or prospective study would be one step in validating whether or not chronic low-dose radiation exposure is the etiological agent for an increase in morbidity and mortality at a younger age.
Brief Literature Summary
There are a number o f publications on the topic of radiation and radiation protection. Whole professions, organizations and committees have been established to review many aspects of radiation. This includes the profession of Health Physics. the International Council on Radiological Protection (ICRP), the National Council on Radiation Protection and Measurements (NCRP) and the U.S. National Research Council. Also there lire many more publications and journals that devote large sections to studies involving possible health risks associated with radiation. In addition to these sources of information are the rules and regulations that are published in the Code of Federal Regulations (CFR) pertaining to the proper use and transport of all radioactive materials that licensed groups in the United States are required to follow. Included in these rules are occupational exposure limits and exposure limits to the general public. All of these professions. organizations, journals and regulations have one thing in common. and that is acknowledging radiation as a known carcinogen and killer at high dose levels. For the last one-hundred years many studies have reported the deleterious effects of high-dose radiation exposure. Cells exposed to ionizing radiation can develop prolonged genetic instability. This instability Is manifested in many ways. including delayed reproductive death, an increased rate of point mutations, and an increased rate of chromosome rearrangements. It has been suggested that multiple mechanisms, occurring in both entirely and late phases of cell growth. may be involved leading to cancer induction.
For chronic low-dose radiation exposure the evidence of morbidity and mortality is much less conclusive. Nevertheless, the cancer risk from low-level radiation is estimated from the known effects at high dose levels by use of a linear-no threshold hypothesis. Using these estimates, occupational and general public dose limits have been derived. The accepted occupational exposure limit based on a concept known as ALARA, as low as is reasonably achievable, is 5 rem γ-1. For the general public, it Is 0.1 rem γ-1. The occupational dose limit represents a level of exposure that has no clinically measurable effects. However, it has been postulated that chronic occupational low-level exposure to radiation can cause an increase in morbidity and mortality at a younger age.
Two of the classic studies about chronic low-level radiation exposure are by Brown and Doll and by Seltzer and Sartwell. Brown and Doll looked for the cause of mortality in 1,377 male British radiologists between 1897 to 1957. They found that 1I significant excess of cancer deaths occurred prior to 1920. No excess mortality was found among those men entering the practice of radiology after 1920. The findings suggested that appropriate safety precautions were instituted in 1920 that accounted for a decrease in measurable excess mortality from chronic radiation exposure. The study also suggested that due to better radiation safety practices, the long-term risks of radiation exposure were estimated to be minimal. Seltzer and Sartwell looked at the cause of mortality of members of several American medical specialty societies from 1935 through 1958 to test the hypothesis that mortality Is increased by occupational exposure to ionizing radiation. The results indicated that mortality Increased with age, but decreased over time for all except the oldest age groups set up in the study.
There was no excess mortality among radiologists 35-49 years over the period 1945 through 1958, suggesting that the etiological agent (Le., radiation) may have been controlled. The increased morality risk was distributed over a number of assigned causes of death which included cancer, cardiovascular disease, and other diseases. These causes were increased in the study groups with high exposure to ionizing radiation. The paper concluded that exposure to ionizing radiation prior to 1945 had produced a nonspecific life shortening effect in the physicians studied.
Since the 1960’s other studies have focused on 11 possible increases in mortality in radiation workers. An increase in mortality due to leukemia has long been associated with radiation exposure lit high doses. In 1981 , Rinsky et al., explored a reported five-fold increase in leukemia mortality among workers exposed to ionizing radiation at Portsmouth (New Hampshire) Naval Shipyard. The retrospective cohort mortality study investigated three groups of workers at the shipyard based on service of employment. There were 7,615 radiation workers with exposures between 0.001 rem to 91,414 rem, 15,585 non-radiation workers used as an internal control group, and 1,345 radiation workers who received no measurable radiation exposure. Among the radiation workers, the observed number of deaths were within a 95% confidence interval of the expected number of deaths. There was no dose-response relation with radiation associated with leukemia or any increased mortality for tiny reason for non-radiation workers. For several reasons this study did not make a solid conclusion. Among the reasons stated was the fact that a short latency period of 15 years had been used. It was suggested that follow-up continue for another 10-20 years.
In 1982, Dreyer and Friedlander identified health risks from low-dose ionizing radiation. This paper indicated that at organ doses of less than or equal to 50 rad, the only diseases to have been reported consistently were thyroid cancer, salivary gland tumors and leukemia. Salivary gland tumors and thyroid cancer were observed in association with certain x-ray therapies such as epilation of the scalp for tinea capitis. These therapies are no longer employed. However, leukemia was observed to occur at cumulative doses of greater than or equal to 30 rad of low-LET radiation. This study implied that leukemia occurred at low doses of low-LET radiation.
In 1981, Gibbons investigated statistical correlations between cause of death and the cumulative radiation exposures of 8,318 white men who were hired by the Department of Energy’s Oak Ridge National Laboratory in Tennessee between 1943 and 1972. The subjects were studied through 1984; 18% of the subjects died during this period. The risk of dying from cancer was found to increase by almost 5% for each rem of radiation exposure incurred over the course of employment lit the facility. The study also revealed a 63% higher incidence of leukemia than the average U.S. male. However, leukemia risk did not increase as radiation exposure increased, as would have been expected.
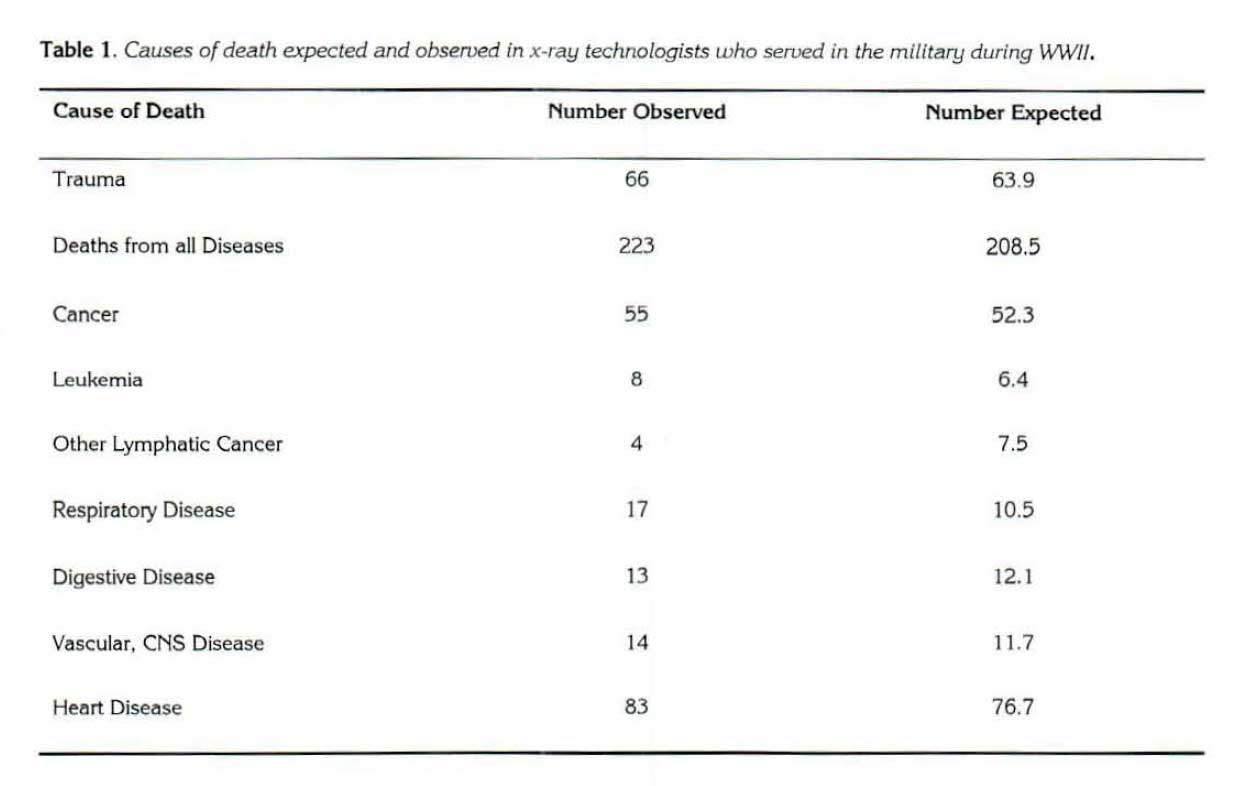
Recently several studies have been published that agree with the classic studies about chronic occupational low-level radiation exposure. In 1991 , Pagel1l1 reported on a study performed by the military that looked at occupationally exposed x-ray technologists who served in World War II. The purpose of the study was to evaluate whether or not an abnormal number of deaths in this group, particularly leukemia deaths, was due to radiation exposure. The study found that none of the observed causes of death, including leukemia deaths, were statistically Significant to warrant concern. (See Table I .)
Death due to respiratory disease was the only category in which the observed number of deaths exceeded the expected by a significant difference. This finding can be attributed to ~ confounding factor of smoking by these subjects, which led to increase in lung cancer.
In 1994, Wiggs et aI., reported a cohort mortality study that was conducted at Los Alamos National laboratory (LANL). A group of 15,727 white men who were employed at the facility were followed for nearly 30 years. The study indicated that no one cause of death was significantly elevated among radiation workers when compared with unexposed coworkers.
Also in 1994, Yalow reported a study about the effects of ionizing radiation. In this study, populations in geographic areas of increased cosmic radiation and high natural background radiation, radiation-exposed workers, patients with medical exposure and those who had accidental radiation exposure were reviewed for possible health effects. There was no evidence of harmful effects associated with increases in background radiation of three to ten times the usual levels. American military personnel who participated in nuclear testing had no increase in leukemia or other cancers. Although this docs not mean that some military personnel are not receiving remuneration for exposure, it refers to the fact that none have excess cancer when compared to the general public. Among 22,000 patients treated for hyperthyroidism with 131I ( 10 rem, mean dose). no increased incidence of leukemia was found. In addition. no increase in lung cancer was found in miners exposed to radon who were non-smokers.
Conclusion
The overwhelming consensus to date is that appropriate radiation safety measures instituted since the end of World War 11 have led to a decrease in 0 Significant number of attributable (clinically measurable) health problems due to low-dose radiation exposure. In 1996, the Health Physics Society reported a new position statement on low-level radiation use and controls. It states that: “In accordance with current knowledge of radiation health risks, the Health Physics Society recommends against quantitative estimation of health risks below an individual dose of 5 rem in one year, or a lifetime dose of 10 rem in addition to background radiation. Risk estimation in this dose range should be strictly qualitative accentuating a range of hypothetical health outcomes with an emphasis on the likely possibility of zero adverse health effects. The current philosophy of radiation protection is based on the assumption that any radiation dose, no matter how small, may result in human health effects, such as cancer and hereditary genetic damage. There is substantial and convincing scientific evidence for health risks at high-dose. Below 10 rem (which includes occupational and environmental exposures) risks of health effects are either too small to be observed or are non-existent.”
Suggestions for Further Study
In reviewing the literature it is obvious that the issue of morbidity and mortality at a younger age due to chronic low-dose radiation exposure is extremely hard to prove. There are many reasons for this, some of which are inherent in any epidemiology study. The role of chance, bias, confounding, strength of association. biologic credibility and consistency with other investigations, till must be proven in order to establish 0 cause-and-effect relationship. I ‘~1 Confounding is hard to prove when dealing with long latency periods, .!IS Is the case when studying chronic low-dose radiation exposure. Many etiological agents (i.e., smoking cigarettes) in addition to radiation have been proven to be carcinogenic. It is possible that chronic low-dose radiation exposure is a contributor to the development of cancer. However, to say that it is the sole reason is hard to ascertain when latency periods to onset of most cancers is twenty to thirty years from exposure. The best gauge for understanding the effects of radiation exposure is consistent retrospective and prospective epidemiological studies that demonstrate chronic low-dose radiation exposure is the cause for morbidity and mortality at a younger age. Therefore, more studies are needed to investigate possible long term health effects from chronic low-dose radiation exposure. This is a long arduous task best done at a national level retrospectively looking at dosimetry reports and death certificates. According to Mayya et al., “computations have been made on the minimum databases required for detecting radiogenic cancer excesses from epidemiological surveys of populations exposed to low-level radiations.” The minimum required database for Western populations is 121,500 person-years. That means in order to have a statistically significant survey one would need to track approximately 6. 100 indtv1duals for about 20 years in order to have 122,000 person-years or about 4.100 individuals for 30 years in order to have 123.000 person-years.
References
1. Murnane, J .P., “Role of Induced
Genetic Instability in the Mutagenic
Effects of Chemicals and
Radiation.” Mutation Research.
367(1), pp. 11-23; 1996.
2. Cohen, B. L., “How Dangerous is
Low-level Radiation?'” Risk
Analysis, Vol. 15, No. 6: pp. 645-
653: 1995.
3. National Council on Radiation
Protection o!Ind Measurements,
NCRP Report No. 116, Limitation
of Exposure to Ionizing Radiation,
Bethesda. MD: pp. J·88: 1993.
4. LaDou, J .. Occupational
Medicine, Norwalk, CT: Appleton
& Lange, pg. 525; 1990.
5. Brown. W.M.C. and R. Doll,
“Expectation of Life and Mort2llity
From Cancer Among British
Radiologists,” British Medical
Journal, pp. 18 1- 187; July 26.
1958.
6. Seltzer, R. and P.E. Sartwell, ‘The
Influence of Occupational Exposures
to Radiation on the Mortality
of America Radiologists and
Other Medical Specialists,”
American Journal of Epidemiology.
Val. 61 . No. I : pp. 2·22;
1965.
7. LaDou, J., Occupational
Medicine, Norwalk, CT: Appleton
& Lange, pp. 197-198; 1990.
8. Rinsky R.A. , RD. Zumwalde, R.J.
Waxweiler, W.E. Murray, Jr. , P.J.
Beirbaum, P.J. Landrigan, M.
Terpilak and C. Cox. Cancer
Mortality at a Navy Nuclear
Shipyard,” The Lancet, 1(82 14):
pp. 231-5; January, 1981.
9. Dreyer NA and E. Friedlander,
“Identifying the Health Risks From
Very Low-Dose Sparsely Ionizing
Radiation. H American Journal of
Public Health. 72(6): pp. 585-588;
1982.
10. Gibbons. W., “Low-Level Radiation:
Higher Long-Term Risk?”
Science News. 139: pg. 181;
March 23, 1991.
11 . Page, W.F. , Epidemiology in
Military and Veteran Populations,
National Academy Press. pg. 88;
1991.
12. Wiggs. L.D., E.R. Johnson, CA.
Cox-DeVore and GL Voelz,
“Mortality Through 1990 Among
White Male Workers at the Los
Alamos National Laboratory:
Considering Exposures to
Plutonium and External lonizing
Radiation.” Health Physics. 67(6):
pp. 577-588; 1994.
13. Yalow, R.S”., “Concerns with Low-Level
Ionizing Radiation.” Mayo
Clinic Proceedings. 69(5): pp.436·
440; 1994.
14.Mossmnn K.L, M. Goldman, F.
Masse, W.A. Mills, K,J. Schiager
and RL Vetter. Radiation Risk in
Perspective – Health Physics
Society Position Statement,
http://www.sph.umich. edu
%7Ebbusby/Hprisk.htm
15. Hennekens. C.H. and J.E. Buring,
Epidemiology In Medicine,
Boston: Liltle, Brown ond
Compo!lny, pp. 30-<12: 1987.
16. Mayya Y.S., P.V. Joshi and K,S.
Nambi, “Database Requirements
for Epidemiological Estimates of
Radiation Risks in Continuously
Exposed Populations. ” Risk
Analysis, 14(5): pp. 829·831 ;
1994.
About the Author
Norman E. Bolus received BS degrees in Biology and Nuclear Medicine Technology from the University of Alabama lit Birmingham. He expects to receive an MPH degree in Occupational Health and Safety in 1998 also from the University of Alabama at Birmingham. For three years. he held a sto!lff position at the University of AllIbllma Hospital in the Nuclear Medicine Department as o!I certified nucleZlr medicine technologiSt. In 1992. he transferred to a teaching position within the School of Health Related Professions where he presently works. Mr. Bolus is an o!Ictive member of the AlabZlmZl Society of Nudeo!lr Medicine where he is currently the President-Elect for 1997-1998 and will be President in 1998-1999. The University of Alabama at Birmingham School of Health Related Professions, Building 333 1714 Ninth Avenue South Birmingham, AL 35294-1270